With soft contact lens (SCL) design, the two factors that can greatly contribute to the lens-to-ocular surface relationship are the lens base curve and the diameter. Together, the base curve and diameter are directly linked to the sagittal depth of a soft contact lens. Adjusting the sagittal depth may improve centration and on-eye performance of a soft contact lens.
The contemporary, widely manufactured hydrogel and silicone hydrogel lens designs are optimized for comfort and to match the corneal and scleral shape of the average eye. We have all seen patients with end-of-day discomfort or who are wearing soft lenses that exhibit inadequate coverage past the limbus. Patients who believe that they are not able to wear contact lenses also present in our exam chairs. Two questions often cross our minds: 1) How can we optimize our chair time and effectively select soft contact lens options for these individuals? And 2) How do we efficiently determine whether patients require a custom soft contact lens to best fit their ocular surface?
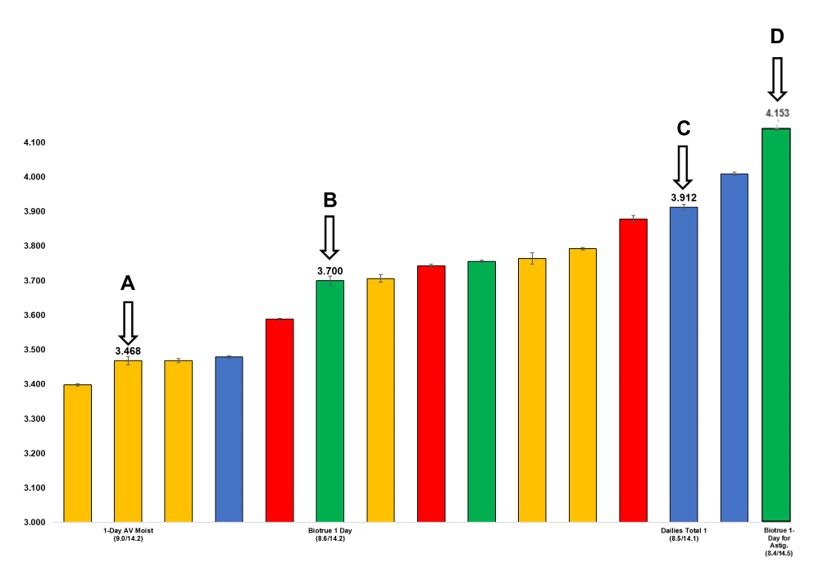
In a recent publication in Contact Lens and Anterior Eye, van der Worp et al. reported the sagittal depths of a series of modern commercially available soft contact lenses. The sagittal depth charts have provided some insight into answering these questions and have helped guide our clinical decision-making. To demonstrate how we apply the sagittal depth charts to clinical practice, we present the case report below.
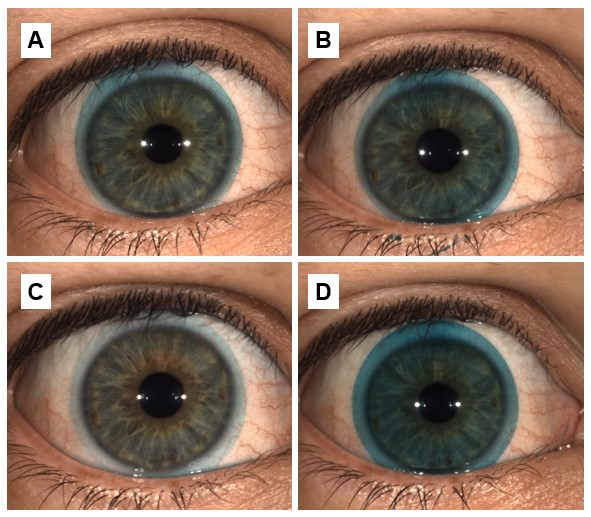
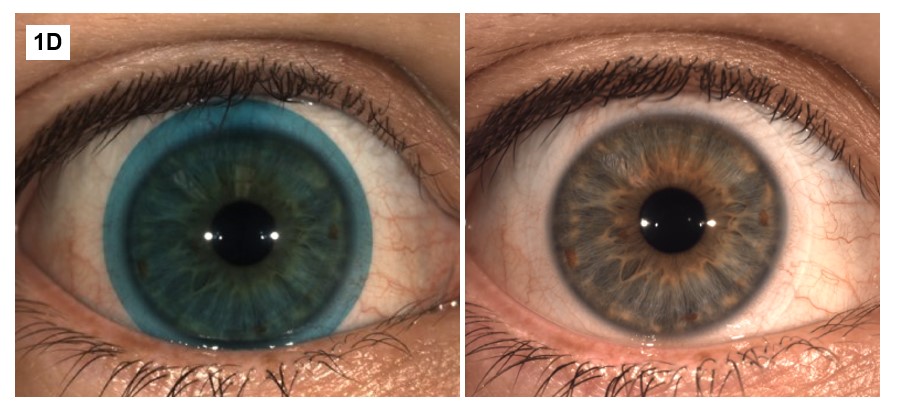
The patient in Figure 1 is a 23-year-old optometry student who has struggled with soft contact lens comfort and reports that his eyes are irritated after a few hours of lens wear. The patient was interested in wearing daily disposable lenses, if possible. Figure 1A reveals a shallow-fitting lens on the patient’s eye, with inadequate limbal coverage and superior-temporal decentration of the lens on eye. To improve the contact lens fit, the patient requires a deeper lens with a higher sagittal depth. To observe a change in the SCL fit, we predict that the contact lens sagittal depth requires an adjustment of approximately 250 microns. The lens in Figure 1B is 232 microns deeper than the lens in 1A, resulting in a slight improvement in lens centration but still inadequate coverage of the SCL past the limbus. Yet again, we need to apply a lens that has a greater sagittal depth, in this case greater than 3700 microns (sagittal depth of lens 1B). Although the ideal next lens would have a sagittal depth of approximately 3950 microns, lens 1C was the deepest spherical daily disposable lens available at the time of the CL fitting (212 microns deeper than lens 1B). Figure 1C shows adequate centration, lens movement, and approximately 1mm of limbal coverage. The patient reported that lens 1C was the most comfortable spherical daily disposable trialed. The patient’s spectacle prescription is -3.00 -0.75 x 180, but he has habitually worn the spherical equivalent CL Rx of -3.25DS. Low-cylinder lenses can sometimes offer an advantage in fitting individuals similar to our patient, as the toric lens counterparts often have a larger lens diameter and therefore a higher sagittal depth. Figure 1D shows a toric lens that is 241 microns deeper than lens 1C. Although the fit seems relatively similar to 1C, the patient reported improved comfort and appreciated the vision with the astigmatism-correcting optics. The patient determined that lens 1D provided acceptable comfort, but he was interested in pursuing other SCL options due to continued lens awareness.